Nicky Snazell's award-winning Physiotherapists Stafford, we provide physio services to areas including Stafford, Litchfield, Cannock, Rugeley & Uttoxeter. Call us today or use the form on this page to get in touch. Our team are here to help at 01889 881 488.
The big toe joint at the base of the big toe can be damaged when the foot is jammed into the ground – such as when pushing off for running – resulting in forced over straightening (hyperextension) of the joint. Typical symptoms include pain at the base of the toe.
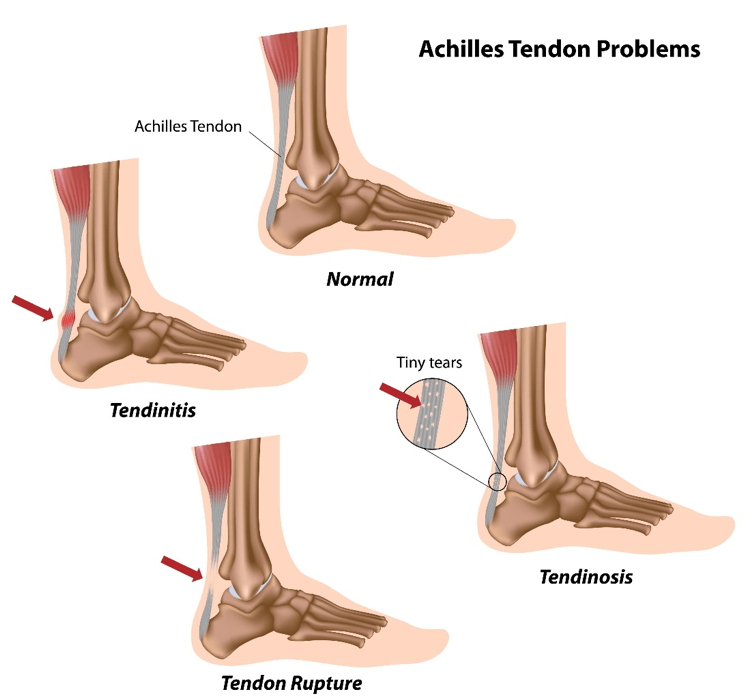
Achilles tendinitis is the irritation/inflammation of the large tendon at the back of the ankle. This is an acute condition, rather than the chronic condition called tendinosis. Causes of achilles tendinitis include a lack of flexibility and overpronation, increasing running mileage, more uphill work, poor footwear, and poor biomechanics.
Typically the back of the ankle is very sore after rest, about 4 cm above tendon insertion on the heel bone (calcaneus). Pushing off through the foot will also be difficult. Rehab must allow for adequate rest to stop the tendon getting inflamed. Initially, cycling and swimming is progressed to weight bearing and balance exercises, and then plyometrics. Diagnosis is by physiotherapy assessment, biomechanical assessment, and MRI scan, and treatment can include: sports rehab exercises, stretches, a training program, MBST, orthotics, physiotherapy, massage, and laser. For chronic cases, Gunn IMS and shockwave will be needed.An increase in running mileage, more uphill work, poor footwear, and poor biomechanics can cause this. Like with Achilles tendinitis, the back of the ankle is very sore after rest, about 4 cm above the tendon insertion on the heel bone (calcaneus). Pushing off through the foot will also be difficult.
Rehab must allow for adequate rest to stop the tendon from getting inflamed. Initially, cycling and swimming are progressed to weight-bearing and balance exercises, and then to plyometrics.
Diagnosis is based on physiotherapy and biomechanical assessments, and MRI scan, and treatment can include: sports rehab exercises, stretches, a training program, MBST, orthotics, physiotherapy, massage, and laser; for chronic cases, Gunn IMS and shockwave.
The two peroneal tendons – the brevis and longus – run outside the lower leg and then behind and underneath the bony prominence on the outside of the ankle (lateral malleolus). A high arch tends to increase the stress through the tendons and thus aggravate the condition.
Peroneal tendinitis is a chronic wear-and-tear problem resulting from repetitive loading, and in some cases, the tendons can become torn. Symptoms of peroneal tendinitis include pain and inflammation on the outside rear of the ankle. This inflammation will cause stiffness, especially after periods of inactivity, such as first thing in the morning.
The tendons are activated in direction changes, and therefore sports involving rapid changes of direction will aggravate the tendinitis and should be avoided while healing. Biomechanically, a high arch with an inverted ankle (the foot being rotated as if you are trying to look at the bottom of your foot) will predispose you to peroneal problems. A complete tear would be evident, as you would not be able to move the foot to the side. Occasionally, nearby nerves (sural) are affected, which can cause nerve hypersensitivity.
Diagnosis is based on physiotherapy assessment, peroneal tendon testing, and biomechanical assessment for overpronation and excessive eversion. Treatment can include: biomechanical assessment, orthotics to assess whether the high arch is a problem, foot plate analysis to assess pressure around the big toe, rehab with strengthening and stretching of the peroneal and calf muscles, and sports.
The peroneal nerve branches off the sciatic nerve and is responsible for innervating the muscles that raise the foot and toes. Damage to the nerve can thus lead to spontaneous foot drop or weakness in lifting the foot. Other symptoms include a tingling or numbness on the outside of the lower leg, and pain down the shin or the top of the foot.
Peroneal nerve injuries have a poor chance of recovery, worsening with time, so it is important to be assessed quickly by a specialist who can determine whether to proceed with surgery or go down a more conservative route – typical conservative options include physiotherapy and orthotics.
Diagnosis is by EMG tests, an orthopaedic surgeon, or a back specialist, and treatment can include: Gunn IMS for assessment, physiotherapy, and biomechanical assessment.
Achilles tendinitis is the irritation/inflammation of the large tendon at the back of the ankle. This is an acute condition, rather than a chronic condition called tendinosis. Causes of Achilles tendinitis include a lack of flexibility and overpronation, increasing running mileage, more uphill work, poor footwear, and poor biomechanics.
Typically the back of the ankle is very sore after rest, about 4 cm above tendon insertion on the heel bone (calcaneus). Pushing off through the foot will also be difficult. Rehab must allow for adequate rest to stop the tendon from getting inflamed. Initially, cycling and swimming is progressed to weight bearing and balance exercises, and then plyometrics.
Diagnosis is by physiotherapy assessment, biomechanical assessment, and MRI scan, and treatment can include: sports rehab exercises, stretches, a training program, MBST, orthotics, physiotherapy, massage, and laser. For chronic cases, Gunn IMS and shockwave will be needed.
An increase in running mileage, more uphill work, poor footwear, and poor biomechanics can cause this. Like with achilles tendinitis, the back of the ankle is very sore after rest, about 4 cm above tendon insertion on the heel bone (calcaneus). Pushing off through the foot will also be difficult.
Rehab must allow for adequate rest to stop the tendon getting inflamed. Initially, cycling and swimming is progressed to weight bearing and balance exercises, and then plyometrics.
Diagnosis is by physiotherapy assessment, biomechanical assessment, and MRI scan, and treatment can include: sports rehab exercises, stretches, a training program, MBST, orthotics, physiotherapy, massage, and laser, and for chronic cases, Gunn IMS and shockwave.
Do you have leg pain, but no amount of working your leg muscles or prodding specific places gives a pain? If so, you may have radiculopathy (see the spinal section).
Do you have pain and swelling over the outside of the ankle, which gets worse with activity? If so, you may have peroneal tendinitis or a peroneal nerve injury (weakness of foot raise).
The two peroneal tendons – the brevis and longus – run outside the lower leg and then behind and underneath the bony prominence on the outside of the ankle (lateral malleolus). A high arch tends to increase the stress through the tendons and thus aggravate the condition.
Peroneal tendinitis is a chronic wear-and-tear problem resulting from repetitive loading, and in some cases, the tendons can become torn. Symptoms of peroneal tendinitis include pain and inflammation on the outside rear of the ankle. This inflammation will cause stiffness, especially after periods of inactivity, such as first thing in the morning.
The tendons are activated in direction changes, and therefor,e sports involving rapid changes of direction will aggravate the tendinitis and should be avoided while healing. Biomechanically, a high arch with an inverted ankle (the foot being rotated as if you are trying to look at the bottom of your foot) will predispose you to peroneal problems. A complete tear would be evident, as you would not be able to move the foot to the side. Occasionally, nearby nerves (sural) are affected, which can cause nerve hypersensitivity.
Diagnosis is based on physiotherapy assessment, peroneal tendon testing, and biomechanical assessment for overpronation and excessive eversion. Treatment can include: biomechanical assessment, orthotics with a view to looking at the high arch being a problem, foot plate analysis for pressure around the big toe, rehab with strengthening and stretching the peroneal and calf muscles, and sports.
The peroneal nerve branches off the sciatic nerve and innervates the muscles that raise the foot and toes. Damage to the nerve can thus lead to spontaneous foot drop or weakness in lifting the foot. Other symptoms include tingling or numbness on the outside of the lower leg and pain down the shin or the top of the foot.
Peroneal nerve injuries have a poor chance of recovery, worsening with time, so it is important to be assessed quickly by a specialist who can determine whether to proceed with surgery or go down a more conservative route – typical conservative options include physiotherapy and orthotics.
Diagnosis is by EMG tests, an orthopaedic surgeon, or a back specialist, and treatment can include: Gunn IMS for assessment, physiotherapy, and biomechanical assessment.